Procedures
Laparoscopic Inguinal Hernia Repair Consent Form.pdf
Position: Both arms tucked 
Port Placement: infraumbilical 12 mm port, followed by two 5 mm Pedi ports, one on each side lateral to the rectus muscles, at the level of the umbilicus.

Instruments: 2 duckbills, endoshears, endotacker, endopeanut
Steps:
-
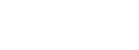
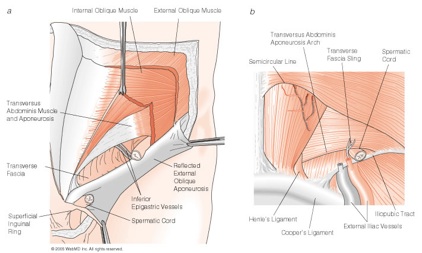
1.Identify the pubic symphysis and the anterior superior iliac spine (ASIS) from the outside of the patient and the inside.
-
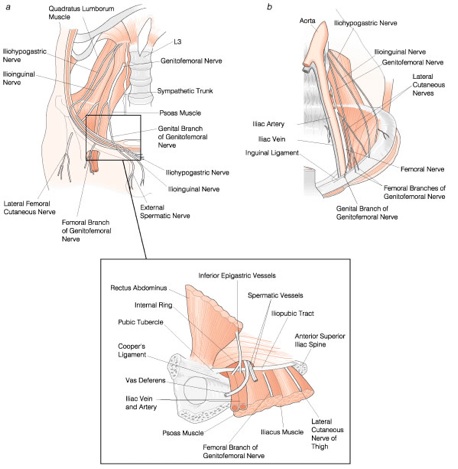
2.Identify the median and the medial ligaments, as well as the major vessels: iliacs, epigastrics (IEV) and gonadals. Identify the hernia defect to determine whether it is direct, indirect or femoral.
-
3.Identify the triangle of doom and the triangle of pain:
-
a.Triangle of doom:
-
1.Borders : vas deferens (VD), gonadal vessels, peritoneal reflection
-
2.Significance: contains the external iliac artery and vein.
-
b.Triangle of pain:
-
1.Located between the iliopubic tract and the lateral aspect of the spermatic vessels. It the region lateral to the deep inguinal ring
-
2.Significance: injury to the lateral cutaceous nerve of the thigh (LCNT) and the genitofemoral nerve
-
-
4.Using endoshears, start cutting the peritoneal layer horizontally starting from the ASIS. Stay superficial so as to avoid cutting into any of the major vessels. Extend the dissection up to the median ligament.
-
5.Using the endopeanut, bluntly dissect the peritoneal layer, reflecting it inferiorly.
-
6.Separate the elements of the spermatic cord from the peritoneal sac bluntly
-
7.Mesh placement:
-
a.Type of mesh: Parietex polyester mesh (see fig)
-
b.Roll the mesh and insert it into the 12mm port
-
c.Lay the mesh out so that the reflection line of the mesh is aligned with the inguinal ligament
-
d.Use the endotacker to secure the mesh to the pubic symphysis medially and the ASIS laterally
-
8.Cover the mesh with the peritoneum and tack it down.
DO NOT USE EXCESSIVE TACKS AND BEWARE OF THE TRIANGLES
Isam Nasr, MD
Objectives: Dissect out cord structures (males) or round ligament (females), identify hernia sac, repair defect with mesh
Lap inguinal hernia repair (TAP)
Saturday, January 16, 2010