If you're looking for the Pittsburgh Mercy Health System Emergency Departments' Intranet web site, it is available here.
If you're looking for my RSI (Rapid Sequence Intubation) or ACLS pocket cards, or my treatise on ABGs, you can find them on the Pittsburgh Mercy Health System Emergency Departments' web site.
EMTALA is an unfunded mandate that basically requires all hospitals in the U.S. to take care of emergency patients properly regardless of ability to pay. Given it's a Federal law, it's also a wee bit more complicated than that. Indeed, many people sit up nights trying to figure out what it really means. I think I've finally got it figured out, at least from a physician's viewpoint. Please peruse the pdf file of this extensive EMTALA article for physicians, with clickable links to the references. Took me about 2 years to write this, but at least for this particular moment (June 2003) it seems to be up to date.
 Now available by mail!
Now available by mail!What? Let me explain.
The Appalachian Search and Rescue Conference uniform shirt is supposed to have a patch on the right shoulder showing your level of medical training.
When I moved to Pennsylvania, I was told that, as a physician, I couldn’t also be a paramedic. Hmph. (They recently relented and said I could take the National Registry exam so I can get back an EMT-P certification, but never mind.) So I followed the state’s directions, took the EMT-Basic skills exam, took the EMT-P written exam, and was issued a certificate and patch as a "Health Professional - Physician." Actually, the patch just says "Health Professional" and nothing about being a physician. And it’s not partcularly pretty compared with many other state’s EMS patches—my favorite is the second version (not the current, third version) of the Virginia EMS patch.
Long ago I’d made up some simple "M.D." patches to wear
on my right shoulder, but now I’m out of them. So I designed an "emergency
physician" patch based on the old Virginia EMS patch. I tried to find
someone else, someone with a related business, to sell these patches, but
failed. I ended up ordering 100 of the MD emergency physician patches
from:
Bob & Bob
P.O. Box 441
Lewisburg, WV 24901
1-800-262-2283
1-304-772-3074
My original order several years ago was for 100 patches for a total of $240 plus $6.50 shipping and handling,
my more recent order cost $212.00 + $5.00 shipping. (I think it was cheaper as
they already had the template.)
Recently (February 2003) I ordered some more, and when I posted a message that they were available again, also with a plea for someone, ANYone, to get me out of the retail business, Lou Jordan and crew, stepped up and offered to sell them. I doubt they will make much money on them, so my thanks to Lou for offering this service to the EMS physician community. Patches are now available from :
Click on the icon for a bigger picture, or here to see the complete design for a similar patch for DOs, ready to send in to Bob and Bob; please use the diagrams to make patches as you see fit, although it'll probably be easier and cheaper overall to get them from the above address. BTW, the patches look very nice -- even better than I expected when I ordered them. Here's a scan of an actual patch:

And if you decide to get some of the DO patches made, please email me as there are a few DOs who are interested.
One of my jobs is teaching emergency medicine residents. A lot of this is bedside teaching, and I give lots of lectures on different topics, one of which is "emergency medicine core content" -- basically, the kind of stuff you find in the various emergency medicine compendium textbooks. I like to use PowerPoint presentations for larger audiences, and Socratic discussions for smaller groups. For emergency medicine core content, at least at our 4.5-hour-long Grand Rounds, seems to work best in Socratic format (mostly because most of the other presentations use slides and it's easier to stay awake with the lights on.) Some residents have found it useful to review my little lecture notes, so I put them online. These are formatted to print out and cut out to 3"x5" size, suitable for putting in a pocket as a quick reference while lecturing. These are somewhat cryptic and designed for me - it's not a substitute for the texts - but if you want a quick review on a topic, with the most important stuff from the current textbooks, with a bit of more recent information and some personal observations and some clinical pearls, here they are. As it's a standard part of emergency medicine residency education these days, I'll also be adding ATLS lecture notes as I make them.
Hospitals need emergency lighting. Yes, there are generator backups, but sometimes even those go out. And, in today's world, planning for REALLY BAD disasters is considered a good idea (some of us were arguing for this decades ago but nobody paid attention). You can indeed put emergency battery-powered lights in the hallways and stairwells, ones that come on with a power outage. But those are really only good for guiding people to the exits, and you need lighting at the nurses' stations, and task lighting for patient care and procedures.
Yes, there are standard commercial lights available for this, but truly, task and area lighting have changed a lot in the past decade or two, and especially in the past year or so (it's mid-2003 as I write this). In particular, disposable lithium batteries and high-efficiency white LEDs have revolutionized lighting in general. You can even get LED replacements for your car's taillights! And, if we're looking for lights that (1) aren't too expensive, (2) will work reliably after being stored in a box for 10 years, (3) will continue working if you drop it, and (4) work for a long time--well, if you're looking for lights like this, forget the traditional NiCd rechargeable batteries (which require careful care and feeding, and often don't work when you take them out of the box) and forget fragile, low-efficiency, short-lived incandescent bulbs. Click on the heading above for more detailed thoughts and recommendations on portable lights for your hospital.
In 1991, I tried to persuade my hospital to use the ICS. I failed. But now, the HEICS (Hospital Emergency Incident Command System) is being required. If you're interested, read my old essay on why hospitals should use the ICS,
Click to view the diagram. It is in PNG format, upgrade to latest version of your browser if not viewable. Notes:
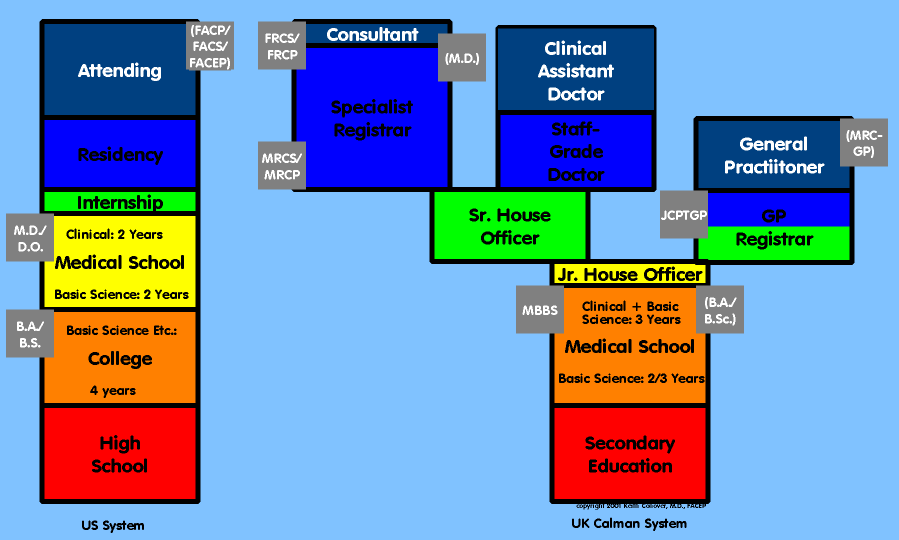
The U.S. has a form of medical training, much-changed from the British version from which it originally derived. The British system is followed in much of the English-speaking world, except for in the U.S. Trying to figure out the parallels is very, very difficult. As some of my British doctor friends where trying to explain it to me, I decided to draw a diagram. First, it was a pair of bar graphs, with 1/4" for each year of training. But as the British types looked at it, they would frown and go "hmm, well, actually. . . " and the diagram got more and more complex. Finally I said "enough!" when one of the doctors was explaining how a qualified G.P. could serve as a Clinical Assistant and wanted my to draw some arrows.
The diagram is of course a gross over-simplification, but as Bacon once observed, we are more likely to learn from error than from confusion.
This diagram shows the new, reformed Calman system of medical education in the British Isles, which is only a few years old. With the old system, you became a Consultant based on who you knew more than anything (the "old boy" network system). This wasn't compatible with the E.U. mandate that doctors, as with other professionals, be able to move between different E.U. countries: thus the Calman commission and its reforms.
Now, if you can get into a Specialty Registrar training program, you are guaranteed to become a Consultant once you get out of Registrarship and pass your exams. The hard part is getting a Registrar position. This is similar to the U.S. system where the hard part is in getting into a residency.
Yes, yes, I know it's not quite precisely right, but if I make it any more complicated people perusing it will lapse into a confused slumber.
Most people who went into emergency medicine, at least back when I started, were frustrated boy scouts (or girl scouts). A deep psychological need to be prepared for just about anything is at the root of this, I think -- whether from bad childhood experiences at being helpless, an intellectual desire to be prepared for the worst, or more likely a combination of the two.
I know that when I was a child, I quit the Boy Scouts because, at least in my area, they were clearly clueless about how to deal with the outdoors. I joined the Potomac Appalachian Trail Club and in particular, its Mountaineering Section -- my parents thought this was fine since I would be with responsible adults -- and indeed some of the finest times of my childhood and early adulthood were with the PATC. (Check out the SAR-outdoor page for more about PATC and such.)
Well, as an ex-Boy-Scout who took the motto "be prepared" to heart, and as an ex-medic, ex-National Park Service ranger, and current emergency physician and SAR team member, I've been carrying some sort of little emergency kit around with me for years. (The only exception is probably when I'm carrying a BIG emergency kit around -- my SAR pack.) And yes, I carry it while running.
As my training and philosophy (and budget) changes, so does the kit. I've finally typed it all up into a single document, and though it will probably change tomorow, I thought it might be nice to share with others of similar inclinations. I hope if nothing else, it stimulates you to put together your own kit. Obviously, the contents will depend on your training, experience, and lots of other things -- but the kit should:
If you have thoughts or comments, feel free to email me.
These three cards are what I made up for myself when a resident and during my early days as an attending. They are primarly for emergency medicine residents to use as pocket references (though the ACLS card may also be of use for nurses and paramedics and other physicians). They aren't copyrighted, and I've posted not only the Adobe Acrobat .PDF files, but also the MS Word 97 "source code" for them so you can take them and adapt for your own use as desired. Important Notes: first, the cards may contain errors or outdated information. Use only if you independently verify every drug and dosage and make sure they're correct, up-to-date, and what you really want to do! Second, the first page of the MS Word file for the CPR card has some section breaks that are invisible, and left over from conversion from another format. So if you try to use the "Page Setup" to change the margins for the first page, it won't work properly. Change the margins for the whole document if you need to, then change the second page as a section.
 ACLS Card
ACLS CardAttending Staff, Information Systems Coordinator, and Director of Wilderness
Medicine Programs,
Department of Emergency Medicine,
Mercy Hospital of Pittsburgh
(full time for about 14 years; well -- actually -- a lot more than full time; but they
only pay me for full time)
 Mercy Hospital is a nice
(well, I think it's nice) non-University but University-affiliated teaching hospital. It's
a "tertiary care center" which means that it takes care of complex patients, but
not quite so complex as the main University of Pittsburgh Medical Center (UPMC). Actually,
for me in the ED that's better, because I don't see so many liver transplants and such,
and I think we see a better population (more interesting medically) at Mercy than they do
at "Presby." (Officially it's really all UPMC rather than "Presbyterian
University Hospital" but everyone still calls UPMC "Presby.") Mercy, along
with UPMC and Allegheny General Hospital, is a Pittsburgh Level I Trauma Center. Mercy
also has a Burn Unit; the other Burn Unit in Pittsburgh is at WestPenn Hospital. Mercy's
ED is the major teaching site for the University of Pittsburgh Affiliated Residency in
Emergency Medicine, and I and the other EMAP doctors are deeply involved in teaching
residents.
Mercy Hospital is a nice
(well, I think it's nice) non-University but University-affiliated teaching hospital. It's
a "tertiary care center" which means that it takes care of complex patients, but
not quite so complex as the main University of Pittsburgh Medical Center (UPMC). Actually,
for me in the ED that's better, because I don't see so many liver transplants and such,
and I think we see a better population (more interesting medically) at Mercy than they do
at "Presby." (Officially it's really all UPMC rather than "Presbyterian
University Hospital" but everyone still calls UPMC "Presby.") Mercy, along
with UPMC and Allegheny General Hospital, is a Pittsburgh Level I Trauma Center. Mercy
also has a Burn Unit; the other Burn Unit in Pittsburgh is at WestPenn Hospital. Mercy's
ED is the major teaching site for the University of Pittsburgh Affiliated Residency in
Emergency Medicine, and I and the other EMAP doctors are deeply involved in teaching
residents.
 The Cathedral of Learning at the University of Pittsburgh
The Cathedral of Learning at the University of Pittsburgh
What this really means:
 I'm an ER doc. Well, only ER docs get to call ourselves ER docs, the rest of you
are supposed to call us Emergency Physicians. And we work in the Emergency Department, not
the ER. OK, enough of the PC talk [that's politically correct, not personal computer]. BTW
the FACEP after my name stands for "Fellow of the American College of Emergency
Physicians" and is an honorific and not a certification. What this means is that we
specialize in the initial care of:
I'm an ER doc. Well, only ER docs get to call ourselves ER docs, the rest of you
are supposed to call us Emergency Physicians. And we work in the Emergency Department, not
the ER. OK, enough of the PC talk [that's politically correct, not personal computer]. BTW
the FACEP after my name stands for "Fellow of the American College of Emergency
Physicians" and is an honorific and not a certification. What this means is that we
specialize in the initial care of:
One of the problems of emergency medicine and other public safety jobs is that you have to work nights. There are several different theories about the best way to do this -- we currently subscribe to the idea that it's best to do your nights spread throughout the month, one or two at a time. The idea is that, for most of us, we never really get adjusted to nights, so trying to bunch your nights is harder than just doing it once in a while. And I've found that I've adapted (fairly) well to this scheme --- maybe it is because I don't drink any caffeine, or because I've never been on a regular schedule for a job, or both, so that my internal clock is flexible. Here is the text of a memo that I wrote about this to someone in our department, with my theory of how to deal with night shifts.

To learn more about Emergency Medicine (whether you're an EP or not) you can't do better than to point your browser at GEMA, the Global Emergency Medicine Archives, the premier EM Web site: http://gema.library.ucsf.edu:8081/. GEMA also has information about the emed-l emergency medicine discussion list, on which I am active, and back archives of this discussion list. You can also download a copy of my hypertext medical notebook from GEMA -- it shows how you can use simple, cheap computer technology to make an emergency physician's life easier.
You don't get CME credit (yet) from participating in the emed-l list, but this is the best way in the world to stay up on what's happening in emergency medicine. Note that this is a closed list; you have to join to post messages (we were getting too much spam and messages like "my toe hurts, what's wrong with it?").
EMAP:
The Emergency Medicine Association of Pittsburgh
(EMAP) is a physician group, comprised of emergency physicians. EMAP is a faculty
practice plan of Mercy Hospital. We do some other outreach work, too, so you'll find EMAP
doctors at Mercy Providence Hospital on the North Side of Pittsburgh.
During a recent need for recruiting, I wrote the following:
Fair warning: Recruiting message
This isn’t an official message, I’m just one of the worker-bees here and trying to help in the recruiting effort.
The Emergency Medicine Association of Pittsburgh (EMAP) is recruiting clinical-academic emergency physicians to start soon. EMAP staffs two hospital EDs: Mercy Hospital of Pittsburgh, 40,000 visits/year teaching hospital, and Mercy Providence Hospital, a small community and psychiatric hospital. Recruited physicians would be expected to work at both institutions.
Important facts about Mercy Hospital:
Mercy Hospital is a Level I adult/pediatric trauma center and burn center. In addition to the main ED, there is also an Urgent Care Center (fast track) open 12 hours a day, staffed by dedicated EMAP emergency CRNPs or by EMAP physicians, and a Pediatric Emergency Center staffed by pediatric emergency physicians or EMAP emergency physicians 12 hours a day. (There are still plenty of pediatric patients the other 12 hours a day to keep your skills up when you’re in the main ED.) There is also a multiplace hyperbaric chamber (though we may replace that with single-place chambers because of some problems with the contract for the multiplace chamber).
Mercy Hospital is a major teaching site for one of the country’s best emergency medicine residencies; staff physicians have faculty appointments in the Department of Emergency Medicine of the University of Pittsburgh and participate in all Emergency Medicine Residency academic activities.
Mercy Hospital has multiple academic affilications, so staff are expected to teach not only with the University of Pittsburgh affiliated EM residents and medical school students, but also students from Duquesne University and other Physician Assistant programs, and medical students from Pitt, Jefferson Medical College, and from medical schools around the world.
Mercy’s ED has a very active emergency medicine research program, including paid research staff and a number of affiliated graduate and undergraduate students.
Mercy has one of the most active EMS programs in the state— physicians provide online medical direction via UHF radios and two hospital repeaters, which the communications center staff can immediately connect with other radio frequencies or phone lines. Communications center staff handle all logging, so physicians are free to talk on the radio without having to chart on any calls.
Mercy ED physicians, along with other residency faculty, also use handheld radios to supervise residents as they provide medical direction for the City of Pittsburgh EMS system.
The Mercy ED has an ultrasound machine (and credentialing for physicians in ED U/S), a helical CT scanner in the department, and 24-hour in-house attending trauma surgeon coverage (though emergency physicians are also involved in major trauma on a regular basis). We have social workers in the ED 24 hours a day. We have a special award-winning people and program for detecting and managing domestic violence.
We are now adding a computer-based speech-recognition dictation system in both EDs.
Important points about EMAP:
EMAP is officially a faculty practice plan, but operates in a democratic consensus manner—in the past, EMAP has had no written contract with the hospital, nor with its physicians, operating instead on less-formal mutual agreements that have been satisfactory to all.
EMAP emphasizes a feeling of community among its physicians—it’s a nice group to be part of. We aren’t like some community-based groups who "eat what they kill"—which is good, because we pay considerably less than community hospitals, and generally less than other academic EDs. Nonetheless, we generally have attracted top-notch physicians, and indeed the group is thought by many (including many of our residents) to be the most popular place to work in the city.
EMAP expects physicians to be multidimensional: we expect you to do a lot more than just work your hours and teach an occasional class. Each physician has related interests outside the strict confines of "work"— for instance, I do a lot of work with mountain and cave rescue teams and get signficant support and encouragement from EMAP—even though the hours I put in don’t reduce my clinical hours much if it all. I guess we’re a group of workaholics—but generally happy ones.
The Mercy ED, though a teaching ED, is different than many. Attending physicians have always been expected to see every patient seen by a resident, even before the HCFA guidelines made this mandatory elsewhere. Attending physicians are also expected to see a fair number of patients themselves—leaving it all up to the residents is simply out of the question (no sitting with your feet up while the residents see patients). The ED has a great mix of patients—probably the best in the city. All physicians, even the chairman, work at least half-time in the ED seeing patients, and take an equal share of overnights.
Truth-in-recruiting disclosure:
Sounds almost too good to be true? (Except the money, but that’s seldom the most important part of choosing a job.) Then why are we recruiting?
Back about 6 months ago, there was a shakeup in the administration—and the hospital lost money last year. (Hospitals that say they didn’t lose money last year are probably lying.) And based on comparing our ED with community EDs, the administration decided to cut our stipend by 50% without notice. The hospital finally recruited a new CEO, who met with the entire group last week, and we’ve worked out a much better arrangement (comparing us to other teaching EDs seemed to help a lot!) But in the meantime, two of our physicians were already planning to leave to move to different parts of the country to be near family, one of our physicians is also an Air Force Reserve KC-135 pilot and got called to serve in Yugoslavia, and three physicians were unhappy enough about the negotiations with the administration that they decided to go out to community hospitals and make real money. So here’s an opportunity for a few people who feel they might fit in with a bunch of hardworking overachievers who don’t get paid enough but really enjoy their jobs (e.g., most of our physicians get a FACEP or FAAEM in relatively quick order).
If interested, you should contact:
Bruce MacLeod, M.D., FACEP, Chair, Department of Emergency Medicine, Mercy Hospital of Pittsburgh, 1400 Locust Street, Pittsburgh, PA 15219-5166, <bmacleod@mercy.pmhs.org, 412-232-8382
We sponsor the well-received annual conference Hot Topics in Emergency Medicine.
All us EMAPers also hold academic positions in the Department of Emergency Medicine at the University of Pittsburgh. Mercy is one of the hospitals that together with UPMC forms the Center for Emergency Medicine of Western Pennsylvania, which is more or less the same as Pittsburgh City EMS which is more or less the same as the Affiliated Residency which is more or less the same as the Department of Emergency Medicine at the University of Pittsburgh's medical school which is more or less the same as the UPMC ED staff but not exactly <deep breath>. See the EMS Page for an explanation.
{kind=link}